.
“As an undergraduate student in psychology, I was taught that multiple personalities were a very rare and bizarre disorder. That is all that I was taught on ... It soon became apparent that what I had been taught was simply not true. Not only was I meeting people with multiplicity; these individuals entering my life were normal human beings with much to offer. They were simply people who had endured more than their share of pain in this life and were struggling to make sense of it.”
― Deborah Bray Haddock, The Dissociative Identity Disorder Sourcebook
Repressed Memories
{kind=link}
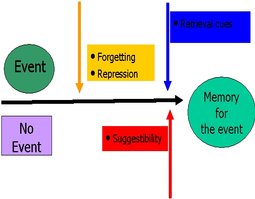
The terms repressed and recovered memories at their broadest refer to memories that were inaccessible until something allowed them to again be retrieved. More specifically, the term "repressed memory" usually refers to the inability to consciously recall a traumatic event, and the term "recovered memory" refers to a traumatic memory that was repressed but is now again accessible. However, the terms “repressed memories” and “recovered memories” are loaded and potentially misleading. There are many theories about what causes traumatic memories to be temporarily inaccessible, including Freudian repression, dissociative amnesia, psychogenic shock, motivated forgetting, directed forgetting, retroactive inhibition, self-induced hypnotic trance states, thought suppression, retrieval inhibition, cognitive gating, or biological protective processes. Additionally, recovered memories of questionable accuracy have been blamed on implanting, personality disorder, false memory syndrome, and suggestion (Dallam, n.d.; Pope, 1998). Some of these theories are better known or better supported than others, and a combination of causes within and across cases is possible.
Among trauma and dissociation researchers, dissociative amnesia is the most studied potential cause of temporarily inaccessible traumatic memories. Under normal circumstances, when an individual encounters new information that is useful or memorable, the information is integrated with the individual’s existing understanding of their self and the world around them. It is theorized that when the individual is under enough stress, this process can be disrupted. Instead of traumatic experiences being stored as memories that feel coherent and part of one’s personal narrative, the sensory, cognitive, and emotional components of the trauma might be stored separately. When the fragments of memory are activated, they are then experienced not as a memory that the individual has control over but instead as intrusions that override an individual’s ability to take context about their present situation into account (Beere, 2009; Nijenhuis, van der Hart, & Steele, 2010; Stern, 2009; van der Kolk & van der Hart, 1991).
According to the theory of structural dissociation, these fragments of traumatic memory are known as emotional parts (EP). When an individual experiences a flashback, one or more EP are intruding on the apparently normal part (ANP), which is the part of the individual that is responsible for functioning in daily life and which experiences these intrusions as distressing and threatening. For individuals with posttraumatic stress disorder (PTSD), the intrusion is usually only partial, and the individual may experience sensations, images, emotions, thoughts, or urges associated with their trauma with or without understanding the context of these intrusions. Sometimes, these intrusions can be more complete, and the EP may overshadow the ANP to the extent that the individual loses awareness of the current date, where they are, or even that the trauma has ended (Beere, 2009; Nijenhuis et al., 2010). Dissociative amnesia can be seen as the inverse of this; when the EP is not present, the ANP has little or no awareness of the traumatic information that the EP holds. In this way, the individual may oscillate between unawareness of the trauma and being overwhelmed by traumatic intrusions with no sense of continuity between these states.
Dissociative amnesia can cover details of a traumatic event, a traumatic event in its entirety, or a series of traumatic events and can range from a sense that the trauma is not personally relevant to the individual (a sense that it occurred to “not-me”) to a complete denial of the trauma. At the most extreme, individuals deny existence of their amnesia because even this knowledge is not integrated into their personal narrative or self concept (Beere, 2009; Nijenhuis et al., 2010), and these individuals may be confused or upset when their amnesia is pointed out to them (Culpin, 1931; van der Kolk & van der Hart, 1991). Finally, an individual may be made aware of their trauma history but then subsequently lose access to this knowledge because it threatens their view of their self, history, and safety (DePrince et al., 2012; Geraerts et al., 2007; Schooler, Ambadar, & Bendiksen, 1997).
Another explanation for why traumatic memories might be temporarily inaccessible is Freudian repression, which hypothesizes that distressing information can be kept hidden from the conscious mind as a way to manage anxiety. According to this model, repressed memories are stored in the unconscious mind, or the id, and the individual must rely on their ego’s defenses in order to keep these memories from surfacing. Traumatic intrusions occur when the memories successfully make themselves known in an attempt to have their associated drives fulfilled. The expectation is that these memories would be the same as any other memory if the individual would stop keeping them suppressed (Stern, 2009). Despite “repressed memories” evoking the concept of Freudian repression, this is no longer a popular model for understanding why traumatic memories might be temporarily inaccessible.
Finally, some researchers are skeptical of the idea that trauma can lead to any differences in how memories are stored. These researches attribute temporarily inaccessible traumatic memories to normal processes of forgetting. They claim that individuals may forget their traumatic experiences due to the passage of time, conscious attempts to avoid reminders of the trauma, or continued suppression of trauma-related thoughts. Under this model, later recollection of trauma is due to cues jogging recall, not special processes of memory recovery (Connolly & Read, 2007; Lindsay & Read, 1995; Loftus, 1993; Patihis & Pendergrast, 2018).
Several factors may encourage memories to be dissociated or forgotten. These include: the nature of the traumatic event; how young the victim was; whether the trauma happened only once (car crash, stranger rape, witnessing a murder) or was repeated (spousal abuse, child abuse, political torture, combat); whether the victim was coerced or explicitly threatened into silence; whether the abuse was sporadically combined with periods of non-abuse ("honeymoon periods"); isolation during abuse; and if a caregiver gave "alternate reality statements" (blamed the victim, denied that anything happened, denied that what happened was wrong) (Dallam, n.d.). One particularly important factor is if the trauma was accidental or impersonal (such as witnessing a natural disaster or a car crash) or a betrayal trauma. Betrayal trauma refers to any trauma in which trust or well-being is significantly violated by people or institutions on which the victim relies for survival. Severe betrayal trauma can result in betrayal blindness, in which the victimized individual turns a blind eye to or forgets the betrayal in an attempt to preserve existing relationships, institutions, or social systems upon which the victim’s well-being depends. Children are especially vulnerable to rejecting awareness of parental abuse because to acknowledge and react to the abuse in a normal fashion would threaten the child's attachment to their parent and so threaten their access to food, shelter, protection, emotional support, or other factors necessary for the child's physical and mental survival (Freyd, 2012). In contrast, children maintaining dissociation from memories or emotions associated with abuse from caregivers can help to preserve attachment and protect social and cognitive development, making dissociation not just necessary but beneficial (DePrince et al., 2012; Fosse, Moskowitz, Shannon, & Muldholland, 2011; Nijenhuis et al., 2010).
Traumatic memories may also be harder to recall because they have low shareability. In particular, child abuse is difficult to talk about, and this may encourage memories of child abuse to be more implicit than explicit, procedural than declarative, perceptual than language based, continuous than categorical, and overall harder to consciously access (Freyd, 2005). There is evidence that when children are not supported by their mothers during or after a trauma, they have a harder time later recalling the trauma. Unfortunately, not only do many mothers disbelieve allegations of sexual abuse in particular, but more severe abuse is associated with a lower chance of maternal belief. This is especially true for mothers who are also being abused, and mothers not speaking about their own abuse can additionally model silence and denial for their abused children. Finally, perpetrators may also discourage the child from speaking about traumatic experiences by grooming the child to view the abuse positively, teaching them to keep silent in order to “protect” the perpetrator or their family, and encouraging the child to blame themself for the abuse. Perpetrators often choose victims whose families can be convinced to disbelieve any abuse allegations that surface, and perpetrators are prepared to react to any accusations by denying the abuse and attacking the credibility of the victim. All of these can make it harder for a child to form a coherent narrative of the abuse and later recall the abuse (Veldhuis & Freyd, 1999). Betrayal trauma, attachment disturbances, and non-discloser of abuse are correlated with dissociation and so may uniquely contribute to dissociative amnesia (DePrince et al., 2012).
Once a memory is less accessible or inaccessible through conscious retrieval processes, conditioning may work to keep it that way. Traumatic intrusions are upsetting to experience, and individuals are motivated to avoid anything that might trigger these intrusions and the dysfunction and emotional pain that they often bring. In contrast, when an individual does successfully keep traumatic memories repressed, dissociated, or inhibited, their ability to retain a more neutral or positive emotional state and their ability to keep functioning in daily life reinforces their desire to continue to avoid anything that might activate the intrusions. The effect of this is often that the individual increasingly avoids anything that might remind them of the trauma, and many survivors learn to rely on dissociation in order to immediately disconnect from the triggers that they are exposed to (Beere, 2009; Elliot, 1997; Nijenhuis et al., 2010). This is why many individuals who have amnesia for childhood abuse are amnesiac for that entire period of their lives (Chu et al., 1999). Unfortunately, this avoidance is often encouraged when others deny the trauma, discourage its acknowledgment or discussion, or shame the survivor for having experienced trauma or for their reactions to the trauma (DePrince et al., 2012).
The separation between awareness of trauma and involvement in daily life may be further reinforced through state dependent learning. Norepinephrine has been linked with flashbacks in individuals with chronic PTSD and so may play a role in activating specific states, such as trauma-oriented states, in structurally dissociated individuals. That is, acute stress that leads to norepinephrine release may be what is needed to activate an emotional part (Nijenhuis et al., 2010), and the traumatic memories may be contained within this dissociated part. State dependent learning has also been linked to different neural conditions during memory formation. One study on fear conditioning in mice found that fear conditioning associations and memories seemed to be only accessible in the physiological state in which the fear conditioning occurred (Jovasevic et al., 2015). Memories can be encoded and stored in completely different neuronal circuits even on a genetic level when the memories are made under different neural states, and this may be what allows some traumatic memories to be inaccessible under normal conditions (Paul, 2015). More information on state dependent learning and its potential role in PTSD, dissociative disorders, and repressed memories can be found here.
Despite all of this, there is some concern, especially among non-professionals, that recovered memories may not be valid. Often, this concern is associated with so-called false memory syndrome and the Satanic Ritual Abuse Panic of the 1980s and 1990s. However, false memory syndrome is not recognized by the American Psychiatric Association although both the DSM-5 and ICD-10 include dissociative amnesia. It must be understood that all memories are to some degree influenced by personal interpretation, and individuals may forget something previously remembered or think that they had previously remembered more than they actually had (Freyd, 2012). There is no support for the idea that recovered memories are any less accurate than continuous memories. The continuity of memories and the validity of memories are two different factors. While it is true that not all recovered memories are accurate, there is no reason to assume that none are accurate. In contrast, there is a good deal of evidence supporting that at least some recovered memories are accurate.
Beere, D. B. (2009). The self-system as mechanism for the dissociative disorders: An extension of the perceptual theory of dissociation. In P. F. Dell & J. A. O’Neil (Eds.), Dissociation and the dissociative disorders: DSM-V and beyond. New York, NY: Routledge.
Chu, J. A., Frey, L. M., Ganzel, B. L., & Matthews, J. A. (1999). Memories of childhood abuse: Dissociation, amnesia, and corroboration. American Journal of Psychiatry, 156(5), 749-755.
Connolly, D. A. & Read, D. (2007). Canadian criminal court reports of historic child sexual abuse: Factors associated with delayed prosecution and reported repression. In M. E. Pipe, M. E. Lamb, Y. Orbach, & A. C. Cederborg (Eds.), Child sexual abuse: Disclosure, delay, and denial (pp. 195-216). New York, NY: Routledge.
Culpin, M. (1931). Recent advances in the study of the psychoneuroses. Philadelphia, PA: P. Blakiston’s Son.
Dallam, S. (n.d.). Questions and answers regarding dissociative amnesia. Retrieved from http://www.leadershipcouncil.org/1/tm/amnesia.html
DePrince, A. P, Brown, L. S., Cheit, R. E., Freyd, J. J., Gold, S. N., Pezdek, K., & Quina, K (2012). Motivated forgetting and misremembering: Perspectives from Betrayal Trauma Theory. In R. F. Belli (Ed.), True and false recovered memories: Toward a reconciliation of the debate (pp. 193-243). New York: Springer.
Elliot, D. M. (1997). Traumatic events: Prevalence and delayed recall in the general population. Journal of Consulting and Clinical Psychology, 65(5), 811-820.
Fosse, R., Moskowitz, A., Shannon, C., & Muldholland, C. (2011). Structural brain changes in psychotic disorders, dissociative disorders, and after childhood adversity. In A. Moskowitz, I. Schäfer, & M. J. Dorahy (Eds.), Psychosis, trauma, and dissociation: Emerging perspectives on severe psychopathology (pp. 159-177). UK: John Wiley & Sons.
Freyd, J. J. (2005). What is shareability? Retrieved from http://dynamic.uoregon.edu/jjf/defineshareability.html
Freyd, J. J. (2012). What is a betrayal trauma? What is betrayal trauma theory? Retrieved from http://dynamic.uoregon.edu/jjf/defineBT.html
Freyd, J. J. (2012). What about recovered memories? Retrieved from http://dynamic.uoregon.edu/jjf/whatabout.html
Geraerts, E., Schooler, J. W., Merckelbach, H., Jelicic, M., Hauer, B. J. A., & Ambadar, Z. (2007). The reality of recovered memories. Psychological Science, 18(7), 564-568.
Lindsay, D. S. & Read, J. D. (1995). “Memory work” and recovered memories of childhood sexual abuse: Scientific evidence and public, professional, and personal issues. Psychology, Public Policy, and Law, 1, 846-908.
Loftus, E. F. (1993). The reality of repressed memories. American Psychologist, 48. 518-537.
Nijenhuis, E.R.S., Van der Hart, O., & Steele, K. (2010). Trauma-related structural dissociation of the personality. Activitas Nervosa Superior, 52(1), 1-23.
Jovasevic, V., Corcoran, K. A., Leaderbrand, K., Yamawaki, N., Guedea, A. L., Chen, H. J., ... Radulovic, J. (2015). GABAergic mechanisms regulated by miR-33 encode state-dependent fear. Natural Neuroscience, 18(9), 1265–1271. doi:10.1038/nn.4084
Patihis, L. & Pendergrast, M. H. (2018). Reports of recovered memories in therapy, informed consent, and generalizability: Response to commentaries. Clinical Psychological Science, 7(1). 32-26.
Paul, M. (2015). How traumatic memories hide in the brain, and how to retrieve them. Northwestern. Retrieved from http://www.northwestern.edu/newscenter/stories/2015/08/traumatic-memories-hide-retrieve-them.html
Pope, K. S. (1998). Pseudoscience, cross-examination, and scientific evidence in the recovered memory controversy. Psychology, Public Policy, and Law, 4(4), 1160-1181. doi:10.1037/1076-8971.4.4.1160
Schooler, J. W., Ambadar, Z., & Bendiksen, M. A. (1997). A cognitive corroborative case study approach for investigating discovered memories of sexual abuse. In J. D. Read & D. S. Lindsay (Eds.), Recollections of trauma: Scientific research and clinical practice (pp. 379-388), New York, NY: Plenum Press.
Stern, D. B. (2009). Dissociation and unformulated experience: A psychoanalytic model of mind. In P. F. Dell & J. A. O’Neil (Eds.), Dissociation and the dissociative disorders: DSM-V and beyond. New York, NY: Routledge.
van der Kolk, B. A. & van der Hart, O. (1991). The intrusive past: The flexibility of memory and the engraving of trauma. American Imago, 48(4), 425-454.
Veldhuis, C. B. & Freyd, J. J. (1999). Groomed for silence, groomed for betrayal. In M. Rivera (Ed.), Fragment by fragment: Feminist Perspectives on memory and child sexual abuse (pp. 253-282). Charlottetown, PEI Canada: Gynergy Books.
This website uses cookies in order to analyze visitor trends. Identifying or personal information is not collected on this website, and the data collected is not sold to or shared with third party services. For more information on the data that this website collects and how to opt out, please visit the Privacy Policy page. Continued use of the website indicates agreement with this policy.
All content on this website is provided for the purpose of general information only. It is not intended to be used as a substitute for professional diagnosis and treatment. Please consult a licensed professional before making any healthcare decisions or for guidance about potential mental health conditions.
This website was last updated 6/22/2024.
This page was last updated 6/1/2019.
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License by Katherine Reuben.